疫情冲击后的医院崩溃在发达民主国家普遍可见;英国BMA主席汤姆·多尔芬称其在2020年“已真正崩溃”,其后“入院到出院”的通道变得更难进入、耗时更长且质量下降。事故与急诊(A&E)前拥堵和转诊延迟已在多国常态化:澳大利亚部分地区近一半救护车患者在A&E外等超30分钟,英国约四分之一(是2019年的两倍),加拿大不少患者甚至离开未就诊的急诊,英国逾四分之一、马萨诸塞州超过五分之一、澳大利亚近一半患者在A&E逗留超4小时;英格兰近十之一急诊入院者约55万人在“推车等待”中超12小时,是2019年的67倍,且“几乎有5000例可避免死亡”与此相关。
择期治疗与专科会诊的积压在持续扩大:有数据显示,11个可统计的经合组织国家中有9个在2024年髋关节置换等待时间仍高于疫情前水平;加拿大2025年专科治疗中位等待期为29周,高于2019年基线约三分之一,并接近2024年创下的30周纪录。牛津大学/约克大学研究者路易吉·西齐利亚尼指出,疫情后等待名单激增与医疗体系的属性(公立或私立)、财政规模、床位与医生密度几乎无显著相关性,说明这是跨国共同的系统性冲击。
“资源增加却效率下降”成为核心悖论:经合组织疫情后卫生支出约占GDP上升到10%左右,欧洲人均支出按不变价已同比增加13%,美国去年新增近14万医疗岗位,英国国家医疗体系自2019年起人员增加25%到约140万人,但总体产能仍未恢复。德国2024年三分之四医院亏损(2019年约三分之一)、美国2025年运营成本上升7.5%(几乎是物价涨幅两倍)且近半增长来自劳动成本(名义增速5.6%);床位占用率长期偏高(美国64%到75%,部分州达88%,爱尔兰94%到96%,英国常在90%)、英国1月治疗等待队列中40%(约280万人)已等超18周,而2019年同期仅57万,形成“排队更久→病情更重→住院更久→进一步堵塞”的恶性循环。

The post-pandemic breakdown of hospital systems is now visible across affluent democracies, with access becoming harder, waits longer, and care less efficient from entry to discharge. After 2020’s suspension of routine care, A&E delays became persistent: in parts of Australia nearly half of ambulance arrivals wait more than 30 minutes, Britain has about a quarter (double 2019), many Canadians leave EDs before being seen, and more than a quarter in England, over two in five in Massachusetts, and nearly half in Australia stay in A&E longer than four hours; in England nearly one in ten emergency admissions—about 550,000 people—waited over 12 hours for a bed, a 67-fold rise since 2019, while the Royal College of Emergency Medicine estimated almost 5,000 avoidable deaths linked to such trolley waits.
Elective-care backlogs remain deep and widespread. In 2024, nine of 11 OECD countries with data had hip-replacement waits above pre-pandemic levels, and Canada reported a 2025 median specialist wait of 29 weeks, more than one-third above the 2019 baseline and near a 30-week record in 2024. A study by Luigi Siciliani found no strong link between post-2020 elective surgery backlog growth and whether systems were public or private, their funding, bed numbers, or physician density, indicating a shared global structural shock rather than a country-specific design flaw.
Meanwhile, health systems show a productivity paradox: OECD spending has moved to around 10% of GDP and Europe’s per-capita real spending is up 13%, while U.S. hospitals added nearly 140,000 jobs last year and NHS staffing rose 25% to 1.4 million, yet output appears weaker. In 2024, three-quarters of German hospitals lost money versus one-third in 2019; U.S. hospital operating costs rose 7.5% in 2025, roughly twice price inflation, with about half driven by labor costs (5.6%), and bed occupancy stayed high (U.S. from 64% to 75%, some states 88%, Ireland 94% to 96%, U.K. around 90%), while 40% of treatment waiters in Britain in January—2.8 million people—had waited over 18 weeks, up from 570,000 in Jan 2019, reinforcing the loop of longer waits, sicker patients, longer stays, and renewed delay.
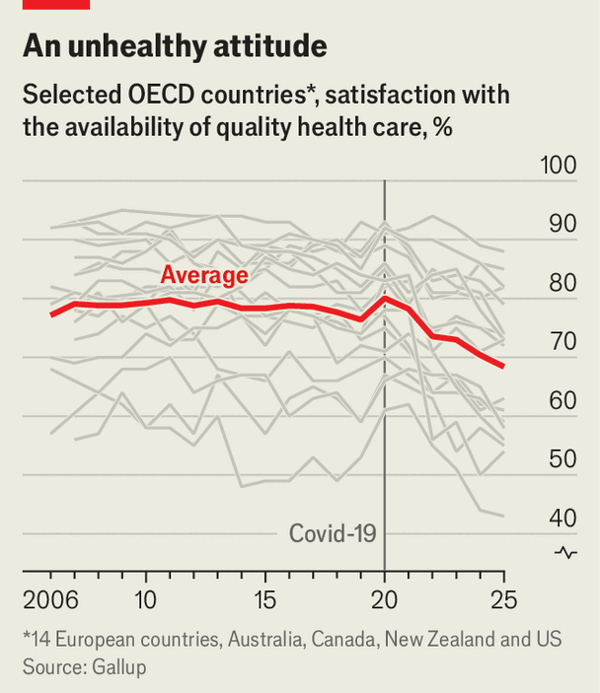
Source: Hospitals never recovered from covid-19
Subtitle: They are stuck in a deadly doom loop
Dateline: 4月 09, 2026 03:57 上午